
Healthcare systems differ widely in financing models, access to high-end technologies and nearly every aspect of care with probably one exception. Paperwork. It is unavoidable and merciless, in the US resident physicians spend an average of 45.6 minutes on the health records per patient. While the average ambulatory encounter runs 15–18 minutes of actual face time.
During a typical outpatient encounter a specialist has to handle history taking, medication reconciliation, orders, chart review, and patient communication. It is hardly surprising that clinicians are blaming red tape as one of the main reasons for burnout.
Luckily, medicine isn’t short on cures. This time remedy came in the form of ambient scribes — digital assistants that take notes so clinicians don’t have to. These tools work by capturing audio of the clinician–patient conversation, transcribing it, then generating a structured draft note.
The first large-scale ambient listening products arrived in 2020, and studies are already reporting reductions in task load and burnout.
This article will:
- review the ambient scribe market in healthcare,
- examine the role of AI in ambient listening tools,
- explore the technical barriers to wider adoption,
- assess how physicians perceive and use them.
Ambient Scribe Market in Healthcare
In the US, Ambient scribes have already turned into a distinct software category. In 2025, the US market for AI in healthcare reached $1.4 billion — scribes alone accounted for $600M, roughly 43% of the total and by far the largest single category.
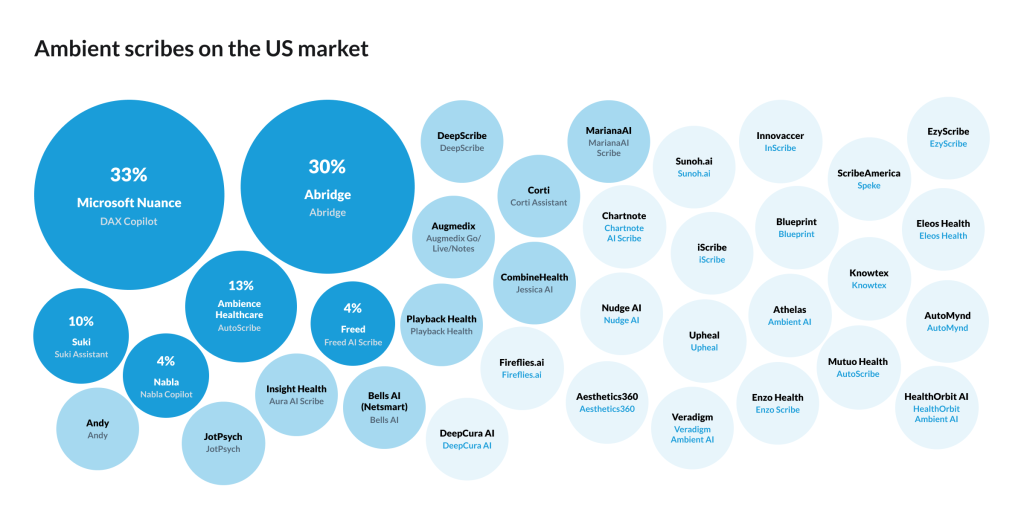
Market shares are mainly divided between Microsoft/Nuance — 33%, Abridge — 30%, Ambience — 13%, Suki — 10%, Nabla — 4%, Freed — 4%.
EHR incumbents are now building native scribe functionality directly into their platforms, for example, Nuance/Microsoft has already deployed its Dragon Medical speech recognition solutions across 77% of U.S. hospitals. By doing so, they convert existing Dragon Medical contracts into DAX Copilot relationships. Oftentimes DAX arrives as an upgrade or add-on to an existing enterprise agreement before the hospital has formally evaluated the ambient scribe market at all. That partially explains their market success.
Nuance keeps its lead through distribution and hospital footprint, while Abridge and Ambience have been taking share by shipping faster and optimizing performance for individual clinical disciplines.
Pricing
Pricing pressure is rising as penetration starts to flatten, hospitals and individual practices tend to switch between providers — vendors are being pushed to lower list prices or absorb costs through deeper discounting. Most vendors do not publicly disclose pricing, striving for multi-year agreements with custom terms, besides, implementation costs are different in every situation. Prices vary, starting from trial tiers broadly available at no cost, with Augmedix listing full-access licenses at $2,400/month per physician.
The table below draws on publicly available data from the major vendors.
Table. Ambient AI scribes. Prices.
| Vendor | Market Share | Monthly Cost | Annual Cost | Notes |
| Microsoft/Nuance DAX Copilot | 33% | $369–$600+ | $8,800–$10,000+ | Setup fee, $650 (first user), $250 (additional) |
| Abridge | 30% | ~$400–$600 (est.) | ~$2,500–$7,200 (est.) | No public pricing; targets health systems of 150+ providers; |
| Ambience Healthcare | 13% | ~$233–$267 (AutoScribe) ~$333–$417 (full suite) | $2,800–$3,200 (base) $4,000–$5,000 (full suite) | No public pricing; tiered bronze–platinum structure; implementation fee on top |
| Suki | 10% | $299 (Compose) $399 (Assistant) | ~$3,600–$4,800 | Volume discounts available; community health centers have received grants to offset cost |
| Nabla | 4% | $0 (≤30 consults/mo) $119 (Pro) | ~$1,430 (Pro) custom (Enterprise) | Free tier confirmed; Pro price widely reported but not officially published |
| Freed AI | 4% | $39–$119 (individual tiers) | $468–$1,428 | Premier at $104/mo billed annually includes EHR push integration; group pricing custom |
About 22% of healthcare organizations have implemented domain-specific AI scribing tools, with adoption highest in health systems at 27% and lower in outpatient providers at 18%.
Adoption rate
Large health system respondents put current ambient scribe adoption at 35% — yet according to Menlo Ventures, that pace is about to stall, and expected to reach only 40% over the next three years.
Several structural factors are likely to hold it back:
- Barriers with workflow integration,
- Resistance to new technology,
- Not all specialties benefit equally,
- Cost constraints.
It is worth noting that healthcare, despite its reputation for institutional conservatism, is outpacing the broader US economy on AI adoption — in 2025 22% of healthcare organisations have deployed commercial AI, while in general, the adoption rate is about 9% across the US economy. So will see how Menlo Ventures’ predictions will play out.
Role of AI in ambient listening
The first generation of tools was, essentially, dictation software. Automatic speech recognition converted spoken words to text with moderate accuracy and no clinical understanding whatsoever.
AI became an enabling technology for scribes, because LLMs can pull clinical structure out of conversational speech, then keep the narrative coherent across sections of electronic health records.
Modern ambient scribing is a pipeline that typically strings together:
- automatic speech recognition,
- diarization — who and when is speaking,
- clinical NLP tuned to particular specialty,
- LLM summarization.
Automatic speech recognition converts audio into text, good enough, but the clinical setting often pushes it into edge cases. There are accents, masked speech, or a mumbling TV in the background. A segmentation step is needed to map free-flowing dialogue into clinically meaningful units and separate clinician’s statements from patient’s. While talking, physicians can add directives – prompts that steer format, verbosity, and where scribes should place details. This is called a summarization-and-structuring pass that turns the transcript into a note. Without AI such speech would end up as a flat word sequence.
Real-world trial data suggests that usability and perceived patient engagement can move even when measured time savings stay modest, which hints that value is partly mediated through attention management during visits rather than minutes saved. In the pragmatic randomised trial, DAX Copilot and Nabla were rated favorably on enabling engagement with patients despite occasional but clinically significant inaccuracies.
One more issue is variability within the medical field — gastroenterology is quite different from cardiology in conversational patterns, making AI scribes uneven in preparedness across specialties. Vendors use this as part of their competitive strategy.
AI also defines what ambient scribes become next. A maturation path started with documentation automation toward administrative actions (letters, forms), then toward reactive and eventually proactive clinical decision support. Scribes are evolving into a platform that can take on adjacent work.
Barriers to Wider Adoption of Ambient Scribes
In America, every note is also a revenue claim. The fee-for-service billing system is built around ICD-10 diagnostic and procedure codes, turning every clinical encounter into a documentation event with direct revenue consequences. More complete notes mean more billable codes, which became an incentive for the $600 million ambient scribes US market to arise. Outside the US, billing architectures are different, reimbursement levers work differently, and the documentation-to-revenue chain is rarely as tight.
Language as an Architecture Problem
Adapting an ambient scribe to a new language requires constructing an entirely new linguistic model from the ground up. Languages could have quite different medical terminology that does not match cleanly — acetaminophen versus paracetamol being the most cited example. To make things worse there are dialects within a single language — a model trained on formal Hochdeutsch will fail in a Swiss-German clinic. And finally the near-total absence of curated clinical speech datasets in many languages.
Patients with non-standard accents or limited proficiency in the dominant training language may receive documentationally inferior care, because the model simply captures their speech less reliably. In clinical trials conducted to date, usage restrictions to English-only visits were imposed because translation capabilities had not been internally validated. Physicians in qualitative studies identified limited functionality with non-English-speaking patients as one of the biggest adoption barriers.
Regulatory Fragmentation Complicates Deployment
The regulatory environment outside the US adds a second layer of complexity that vendors cannot simply engineer around. The EU’s GDPR enforces data sovereignty — voice recordings cannot be freely transmitted to a central US cloud for processing. Vendors are obliged to establish in-country or regional infrastructure, support, active patient consent and a right to erasure.
The UK operationalised this framework in April 2025, when NHS England guidance formally endorsed ambient scribing tools while mandating clinical safety assurance, Data Protection Impact Assessments, and human oversight of all AI-generated content. Similar frameworks are now operative in Brazil (LGPD), South Africa (POPIA), and Saudi Arabia (PDPL), making GDPR-level compliance a global requirement for any vendor with international ambitions.
Beyond data governance, there is the question of device classification. In the EU, if a scribe’s output is used to inform clinical decisions — which is precisely its value proposition — it is likely classified as a Class I or IIa medical device under the Medical Device Regulation, triggering a CE Mark pathway that requires clinical evaluation and an ISO 13485-certified quality management system.

The US FDA operates under considerably more flexible enforcement discretion for basic note-taking functions. The same product that is legally deployable in the US health systems “tomorrow” may require 12 to 24 months of regulatory work before it can reach a European hospital. That’s not all bad news, as within the US itself some states require only one-party consent to record a conversation, while others mandate two-party consent — a distinction that carries direct liability implications.
EHR Heterogeneity as a Scalability Ceiling
A final barrier we would discuss is the EHR fragmentation. The US market is dominated by a small number of vendors, and most major ambient scribes have built deep integrations with them.
Internationally, a single German hospital may run multiple specialised Krankenhausinformationssysteme in parallel. This means rebuilding the product again from scratch. The business model was not designed for that.
Mapping of an ambient scribe output onto the structural requirements of a documentation template directly influences overall accuracy — a variable that multiplies with EHR diversity.
Physicians Perspective On Scribes
Studies consistently show generally positive feedback on scribes from physicians — on work-life integration and overall workload, but perspectives on accuracy and style were largely negative, particularly regarding note length and editing requirements.
“Saves 1–1.5 hours per day and helps clinicians stay more focused on patients during the visit. I would never go back and work at a place that didn’t have this” Admitted an MD on reddit.
Specialists quite quickly devise their own workflow, which saves time and decreases cognitive load: “I dictate my radiology review and lab review into the note prior to seeing the patient, then use it for the patient’s HPI. Then I dictate the assessment plan after the visit.”
Price for a workplace remains a barrier, especially with bigger providers:
“I saw the Dax copilot presentation. I cannot see how this add-on is worth the price they are asking. Any more than $30 in additional monthly fees for Dragon would be excessive. At this point, it does not do enough to justify the cost.”
Hallucinations are common enough to spark dedicated discussion threads on social media asking for the wildest hallucination clinicians have caught:
“[it is hallucinating] Medication, medication route, medication dose, exam findings, symptoms noted as improved when the patient complained of worsening…. And I have a huge instruction text in my template trying to instruct the AI NOT to do this.”
“My favorite was when it said the patient was allergic to meth. Which, fair, but this patient had no history of drug abuse and no allergies, so I have no idea where it pulled that from.”
“I sent a patient from my rural to a tertiary hospital. The note from the accepting physician said “Sent from the fucking hospital” instead of “sent from the (town name) hospital.”