
Have you ever heard a doctor say something like: “Didn’t this help you at all? Hmm. Ok, let’s try these pills instead”? How does it feel to be a lab rat? Of course it’s not human experimentation — but what if you could get the right therapy without all that trial and error? Imagine your doctor had an exact copy of you to test all their ideas on — not on you. Wouldn’t that be fantastic? Today, this isn’t entirely science fiction. You can give your doctor a digital twin to experiment on.
What are Digital Twins in Healthcare
A digital twin for healthcare (DT4H) — is a virtual representation of a person which allows dynamic simulation of potential treatment strategy, monitoring and prediction of health trajectory, and early intervention and prevention, based on multi-scale modeling of multi-modal data such as clinical, genetic, molecular, environmental, social factors etc.
Not the shortest definition, so let’s reach for a practical example of what a DT looks like, and what the technology can do.
Is DT Identical to the Entire Organism?
Not really. DTs range from organ-specific and task-specific to multi-organ composites; whole-body lifetime twins remain a research north star.
Besides, biology is complex, there are always hidden variables and missing mechanisms, so we can only ever estimate closeness to the original within known uncertainty bounds, and closeness to the original is usually defined operationally: how well the twin predicts the real patient’s outcomes under clearly specified conditions. So the model is never identical, it should be good enough to be accurate and trustworthy in a particular scenario.
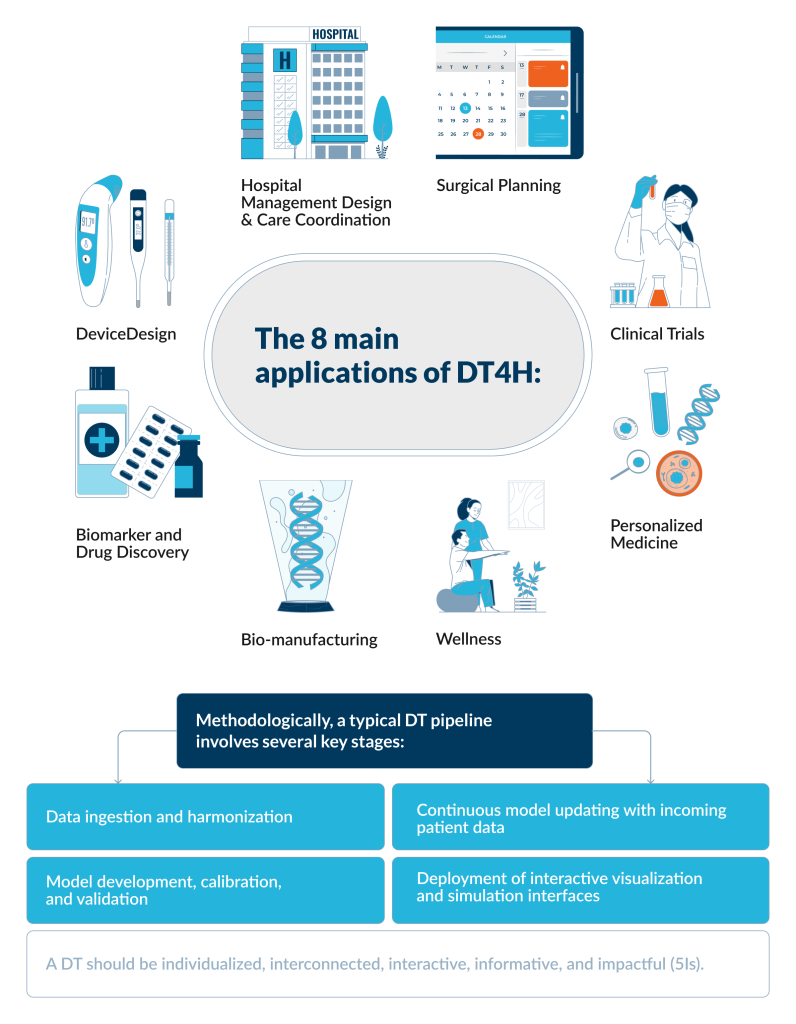
A DT should be individualized, interconnected, interactive, informative, and impactful (5Is).
DTs can become extremely faithful functional replicas for narrow, well‑observed questions:
– Cardiac and electrophysiology DTs can reproduce hemodynamics with errors on the order of 10⁻⁴ in benchmark frameworks and reduce ablation volume while preserving 79% overlap with clinically chosen targets;
– Neuro‑oncology twins have delivered personalized radiotherapy plans that cut dose by 16–17% while maintaining disease control;
- Organ‑on‑chip liver twins can predict human clearance for dozens of drugs better than conventional in vitro models.
Main Applications of DT4H
1. Hospital Management Design and Care Coordination
A hospital bed-flow twin that reallocates beds across specialties to cut waits. A DT is built from real admission/discharge/transfer events and bed-occupancy status, then used to simulate and compare allocation policies before changing operations in the real hospital. In a 2025 simulation-based optimization study using 3 years of admission data, a DT-enabled to reduce the total beds required from 201 to 93; and reduced patient waiting time from 24.38 to 8.80 days.
2. DeviceDesign
Designing a total artificial heart for anatomical fit using virtual patients, before building physical prototypes. RealHeart’s device-design workflow used virtual patient models to evaluate whether design changes improved device fit in the chest cavity by measuring anatomical dimensions and testing fit virtually. In the same RealHeart industry case report, the team states that this approach reduced the need for physical prototyping and helped to decrease the amount of animal studies by resolving fit issues earlier in a simulated environment.
3. Biomarker and Drug Discovery
A single‑cell-based digital twin disease model can prioritize biomarkers and drug targets. A peer‑reviewed approach is to use single‑cell RNA‑seq to build multicellular network models of disease and then use these models to choose candidate biomarkers and therapeutic targets, for example, by prioritizing upstream regulators and disease‑associated genes across cell types and organs.
4. Bio-manufacturing
GSK, Siemens, and Atos piloted a digital twin for vaccine manufacturing that mirrors the process in real time and connects operating conditions to the measured quality of the ingredients. Sensors and process analytical technology provide the live inputs, allowing the model to predict product quality, spot when it is drifting away from the target, and support timely adjustments to process parameters to bring it back on track.
5. Surgical Planning
An anatomic heart digital twin reviewed in mixed reality that changes the surgical plan for complex congenital cases. A national-centre study reports generating 3D anatomic digital twins for 50 patients and presenting them to the heart team after an initial plan was made using standard visualization. In that cohort, the anatomic digital twin changed the initially decided surgical strategy in 68% of cases — an explicit, measurable planning impact.
6. Clinical Trials
Each trial participant can be paired with a model-based twin that estimates how they would progress under standard care, reducing the need to enroll additional placebo/control patients. The same perspective argues this emerging approach could support in‑silico exploration of efficacy and safety signals and, in some settings, reduce required sample sizes and trial timelines.
7. Personalized Medicine
A cardiovascular patient twin that runs what-if simulations to pick an intervention and forecast outcomes. A cardiovascular digital-twin review describes using integrated, streamed multi-source patient data to estimate risk, forecast disease progression, choose an intervention, and predict the likely outcome, i.e., explicit decision support rather than static risk scoring.
8. Wellness
a Fit-twin ingests wearable stream plus context and triggers a specific action when user’s physiology deviates from their own baseline. A published proof‑of‑concept builds a user digital twin using a Fitbit Charge plus an Azure model, and it continuously mirrors the user by pulling wearable data and contextual signals in real time. The twin can interpret whether a deviation is plausibly explained by workout, commute etc. before it recommends an intervention.
Methodology
Many DT Implementations can be Described in terms of standard sequence that starts with data ingestion and harmonization, continues through model development with continuous updating, and ends with interactive visualization and simulation interfaces.
1. Ingestion
A DT pipeline begins by pulling in patient data that already exists in electronic health records, medical imaging, and many other sources and formats. Quite often, these data come in different formats and use different terms to describe the same thing; for example, myocardial infarction may be recorded as “heart attack” or “cardiac infarction.” This defines the need for the second phase: harmonization.
2. Harmonization
Here incoming data is cleaned, standardized, and organized into a coherent dataset. Incoming streams are aligned so that the same clinical concept is understood uniformly throughout the whole process. At this stage happens unit standardization or duplicate handling, also it is important to maintain traceability of the final variables back to their source. Confidence in later simulations depends on being able to explain how each feature was constructed and why it should be trusted.
3. Model building
Model building turns harmonized patient data into a working digital patient: a virtual representation connected to its physical counterpart, designed to run dynamic simulations and generate patient-specific predictions.
In clinical trials for example, the model is trained to project an individual’s likely course under standard of care. That serves as an individualized expected-control trajectory and can be used as a digital comparator in analysis under defined conditions.
4. Calibration and validation
Calibration aligns the model’s parameters with observed data from the real system so its outputs match the system under the conditions it is meant to represent. Teams use historical records and live measurements to tune the model and then run validation on new data to check whether performance holds outside the fitting set. This stage also checks whether the twin behaves plausibly under realistic scenarios.
5. Continuous updating
Personalized models are periodically updated with new patient data, improving predictive accuracy as longitudinal evidence accumulates. Continuous updating is needed to track drift, monitor performance, and manage version changes so that the model is demonstrably better for the intended clinical or research use.
6. Interfaces
The final stage deploys the screens and controls that make the twin usable. A view of the current patient state, the model’s uncertainty, and the outputs of defined scenario runs.
These interfaces are built for iteration. They allow rapid side‑by‑side comparison of alternative assumptions where decisions can be revisited over and over.
DTs are not the new norm yet, but the concept is quite actionable to make a difference to people’s lives. And make news.
JJ’s Case
JJ was born with a complex congenital heart defect, and treated at Boston Children’s Hospital, where clinicians used virtual twin technology to plan highly specialized valve repair. The approach decreased pre-operative uncertainty, allowing to iterate surgical “what-if” scenarios on JJ’s own anatomy virtually.
What the DT enabled that wouldn’t be possible otherwise.
In congenital valve and outflow-tract repairs, surgeons often have to mentally reconstruct 3D spatial relationships and make decisions on the fly in very small patients. Boston Children’s describes using models to sort out the anatomy and guide the operation, run simulation-informed comparisons across candidate repairs, e.g., different ways to form a valve or reroute flow to estimate how each option changes hemodynamics. This also reduced the cognitive load on the team of reconstructing anatomy from memory while the clock is running.
That combination — patient-specific geometry plus simulation-driven “try before you cut” — is the part that doesn’t exist in standard care at the same fidelity: you can’t ethically A/B test multiple surgeries on the same child, and you can’t pause a live operation to explore five alternatives and their downstream flow consequences.
Is it scalable or just a boutique use case?
Boston Children’s surgical leadership describes this approach as a transformation of how they operate, using 3D models to guide operations and applying quantitative planning approaches across large cohorts, reporting over 100 aortic valve patients planned this way already, also they cite being on track for around 630 models in 2025, which is roughly 60% of their surgical volume.
The Role of AI for DT
Digital twins existed long before the invention of AI: “Houston, we’ve had a problem,” was radioed in 1970 during the Apollo 13 mission. Then NASA relied on ground simulators to recreate the spacecraft’s failure modes, test procedures on Earth, and uplink fixes to the crew. To this day, Apollo 13 remains one of the most famous examples of a DT precursor in action.
AI provided an accelerator for components that are computationally intensive or biologically under‑specified, letting the twin run more scenarios, more often, without collapsing under compute cost.
Physics‑based digital twins are built from equations grounded in physical laws. That’s why they can be accurate and scientifically verifiable, but are often slow. Their advantage is credibility, because they can attach confidence limits through uncertainty quantification. AI, in contrast, remains a weaker citizen of high‑stakes medicine: it tends to interpolate better than it extrapolates, where uncertainty quantification is still not broadly established, and most models cannot explain “why,” only “what.” Training data can also be a problem, they can add bias, they are incomplete; skewed datasets can make performance brittle across populations, even as AI is already used to support clinical decisions worldwide.

The forward path described in the paper is “Big AI”: a hybrid framework that blends physics‑based DTs with data‑driven AI so the twin keeps mechanistic discipline while gaining flexibility and speed. In this design, AI frequently becomes the surrogate for the computationally intensive or poorly specified parts of the model, while the physics‑based core anchors predictions to physiology and the scientific method. The result is intended to deliver faster, more reliable, more individualised predictions, authors call it individual “healthcasts”.
The Future of DT
A single universal human DT where the interaction could traverse from microscopic to macroscopic scale and last from birth to death for individuals is not currently practical.
Yet there are audacious programs trying to create integrated Virtual Human Twins.
Initiative from European Commission
The European Commission launched a European Virtual Human Twins Initiative to support the emergence of next‑generation VHT solutions in health and care.
The project aims to build a digital representation of a human health or disease state to refer to different levels of human anatomy, e.g. cells, tissues, organs or organ systems. VHTs are built to mimic and predict behaviour of their physical counterparts, including interaction with additional diseases a person may have.
The main strong side of the initiative — its collaborative nature, the Commission has invested over EUR 100M with main funding provided by the EU, not by business, which allows prioritisation of research goals over profit-driven. Engagement of a Europe-wide platform and federated ICU data infrastructure puts a strong emphasis on interoperability.
Dassault Systèmes: Virtual Twin for Human. Organ-to-human trajectory.
Dassault Systèmes positions its initiative as a journey to model the human body holistically, building on organ programs such as Living Heart and Living Brain and focusing on integrating diverse organ models into one experience.
Operationally, the Living Heart Project is organized as a multi-stakeholder ecosystem, attracting 125+ companies. Dassault states the Living Heart models are intended to serve as a common technology base for:
– Cardiovascular in silico medicine — running virtual experiments on a digital heart to explore interventions and likely responses;
– Medical device design — iterating device concepts in simulation;
– Medical device testing — evaluating device performance in virtual patients, and others.
In its Virtual Human Twin symposium communications, Dassault explicitly states an ambition to create a virtual twin experience of the human body broader than a single organ even if the practical work proceeds organ-by-organ.
We live in a world where the plots of science fiction movies turn into reality faster than they can be written. An anti-utopian future is not the aim of digital twins in healthcare, and it should not become an accidental by-product of scaling data-heavy systems without consent, privacy, and security. There is room for hope and curiosity.