
When a person is placed on a transplant waiting list, time starts moving differently. Life seems to go on, but somewhere in the background there is always a countdown: the constant wait for a call saying that the right organ has been found.
In 2024, a record 173,727 organ transplants were performed worldwide. But there are still not enough organs. And the chance of receiving a transplant depends heavily on the country, the healthcare system, and luck. In the United States, more than 100,000 people are waiting for a life-saving organ. Every day, 17 people die before a matching organ is found.
Different ways of tackling this problem are already beginning to emerge. Scientists are editing pig genomes so their organs become more compatible with humans. Living tissues are being printed using 3D bioprinters. Researchers are attempting to grow human organ structures inside animal hosts. Donor organs are being connected to machines so they do not simply sit on ice, but remain viable outside the body. Mechanical hearts are in development. So are implantable artificial kidneys.
Pig as Donor
Pig organs closely resemble human organs in size and physiology. But the human immune system recognizes a pig organ as foreign and attacks it. For a long time, this looked like an almost impossible barrier to overcome. Then came CRISPR, cloning, and more precise immunology — and the pig went from an “impossible donor” to a bioengineering platform.
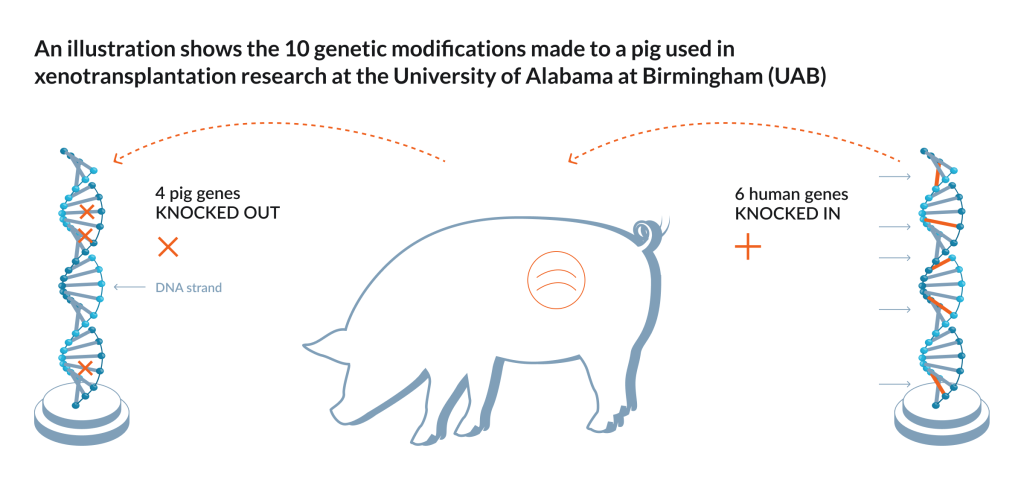
A modern xenotransplant is an animal organ whose genome has been edited in advance. Some genes in pig DNA are switched off because they trigger rejection. Other genes, human ones, are added so the organ looks less foreign to the immune system. eGenesis, for example, engineered a pig kidney with 69 genomic edits for transplantation into a living human patient. United Therapeutics is developing pigs with 10 genetic modifications: six human genes are added, and four pig genes are switched off.
In January 2022, David Bennett received a genetically modified pig heart. He survived for about two months before he died. What mattered scientifically was that the heart was not immediately destroyed by his immune system. In 2023, a second patient, Lawrence Faucette, also received a pig heart. He lived for almost six weeks, and doctors later reported signs of rejection.
In March 2024, 62-year-old Rick Slayman received a genetically edited pig kidney. The kidney began working, and he was discharged from the hospital. Almost two months later, Slayman died, but the hospital said there was no indication that his death was connected to the transplant. Later reports said the cause was an unexpected cardiac episode, not kidney rejection.
In November 2024, Towana Looney from Alabama received a pig kidney with 10 gene edits. The kidney worked for 130 days. Then, because of an infection, doctors had to reduce immunosuppression. Rejection began, and the organ was removed. Timothy Andrews later lived with a similar kidney for 271 days.
Today, the FDA has officially authorized clinical trials of genetically modified pig kidneys in humans, and several companies are planning to scale these transplants to dozens of patients. Many questions remain: rejection, infections, immunosuppression, how long the organ can last, and the ethics of breeding animals as organ donors. But the past few years have shown the main thing: this approach is possible in principle.
Growing a Human Organ Inside an Animal
There is an even stranger approach: growing an organ inside an animal that is made as much as possible from human cells. For example, scientists could take a pig embryo, genetically remove its ability to develop its own kidney, and then add human stem cells. The idea is that an organ suitable for a human patient would begin to grow inside the animal itself.
In 2023, a Chinese research group reported that it had managed to grow early “humanized” kidneys in pig embryos up to day 28 of development. The structure of the organ looked normal, and some of its cells were human. But this was still far from creating a fully formed organ ready for transplantation.
Using this approach, it may one day become possible to take cells from a specific person, return them to a stem-cell state — something scientists can already do — multiply them, and then use them to grow an organ inside an animal for that same patient. The patient might not need to take immune-suppressing drugs for the rest of their life to prevent rejection, because the body would recognize the organ as its own.
Bioprinter: Why Printing an Ear Is Easier Than Printing a Liver
Science fiction films like to show entire organs, and even whole bodies, being 3D-printed layer by layer. Reality is much harder.
Printing living tissue is not like printing a plastic part. You need to place different types of cells in the right positions, create a matrix, provide nutrients and oxygen, ensure mechanical strength, and help the tissue mature. And the biggest challenge is blood vessels. Without a vascular network, a thick piece of living tissue quickly dies: the cells deep inside simply do not get enough oxygen and nutrients. So bioprinting is already producing impressive results, but full livers, hearts, or kidneys for transplantation are not being printed yet.
The first clinical successes are already here, though. In 2022, 3DBio Therapeutics reported the first transplantation of AuriNovo, a patient-specific 3D-bioprinted ear implant grown from the patient’s own cells for microtia — a congenital condition in which the outer ear is underdeveloped or completely absent. This was real living tissue, created for a specific person and implanted as part of an early clinical trial.
And it is a good beginning. First come cartilage, skin, vascular fragments, and mini-tissues for drug testing. Then, more complex structures. Scientific reviews in recent years describe biofabrication as a rapidly growing field: new light-based printing methods are emerging, along with organoids, bioinks, and different ways to control how cells self-organize.
We are not printing full organs yet. But small liver fragments for testing drug toxicity, cartilage for reconstructive procedures, vascular models, and tumor organoids for choosing therapy are no longer science fiction. These intermediate uses are what move the technology toward the larger goal.
There is another route too: take a donor organ, remove its cells, leave behind a “ghost” scaffold made of extracellular matrix, and then seed it with new cells. This is called decellularization and recellularization. After decellularization, a heart or liver looks almost like a glass anatomical model: the shape is still there, part of the vascular architecture is preserved, but the cells are gone. In theory, this scaffold can be repopulated with the patient’s own cells. In practice, it is still difficult. The cells have to attach properly, mature, spread through the structure, and begin working as one system. But recent reviews describe such scaffolds as one of the promising directions in organ engineering, especially for kidneys, livers, hearts, and lungs.
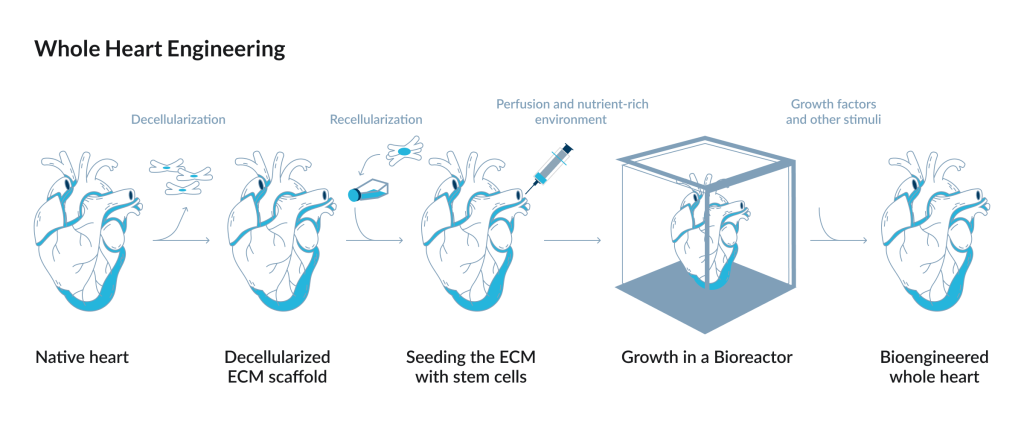
The five-stage process of whole heart engineering, from decellularization of a native heart to the growth of a bioengineered whole heart in a bioreactor.
Source: Barbulescu et al. / International Journal of Molecular Sciences, 2022
So the organ of the future may not be “printed from scratch.” It may be assembled as a hybrid: scaffold, cells, bioreactor, blood vessels, maturation. Not one magic printer, but an entire factory for living tissue.
The Possibility of Restoring an Organ
Instead of growing new organs, medicine can also focus on saving the ones that used to be discarded.
Classical transplantation long worked like a race against time: the organ is removed, cooled, transported, and transplanted. Cold slows down damage, but it does not keep the organ alive. Today, normothermic machine perfusion is being used more often. The organ is connected to a machine, and warm oxygenated fluid or blood containing nutrients and medicines circulates through it. A liver, heart, or lungs can not only be transported this way, but sometimes even treated before transplantation.
For example, the OrganOx metra system for the liver received FDA approval back in 2021, and in 2025 the FDA allowed it to be used during air transport. In this system, a liver can remain viable for longer, doctors can assess it before transplantation, and the distance between donor and recipient becomes less decisive.
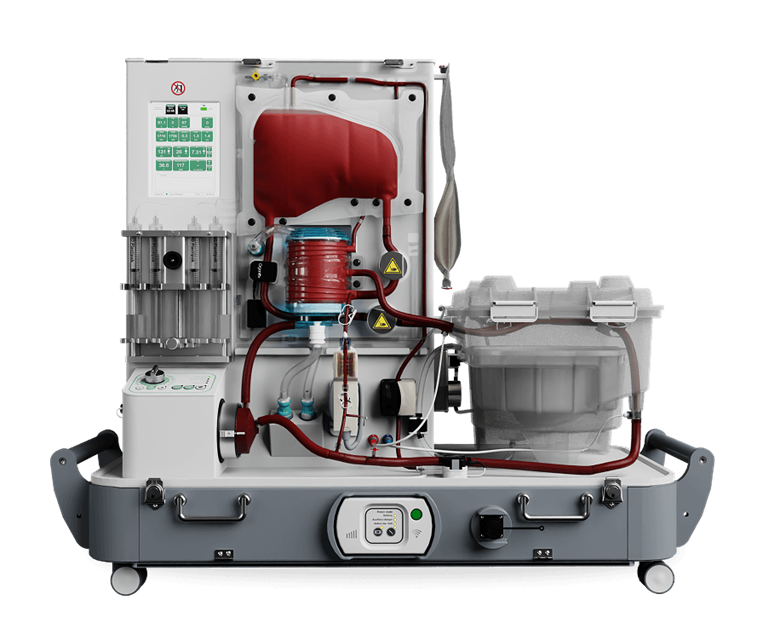
TransMedics is developing a similar idea for the heart, lungs, and liver through its Organ Care System: the organ does not simply sit in a container of ice, but functions in a portable system. In 2026, the company received full FDA IDE approval for the Next-Generation OCS Heart ENHANCE Trial, which studies, among other things, prolonged heart perfusion.
At the edge of this field is OrganEx, a Yale technology that in 2022 partially restored blood circulation and some cellular functions in pig organs one hour after cardiac arrest. It showed that some organs once considered lost may one day be preserved, restored, or prepared for transplantation.
Artificial Heart: An Organ That Does Not Beat, But Saves Lives
If a pig kidney is biology, and bioprinting is engineering with living material, then an artificial heart is pure mechanics. To pump blood through the body, it does not even need to pretend to be human. It does not have to contract rhythmically or look anything like the image of a heart in an anatomy atlas.

In July 2024, the Texas Heart Institute and Baylor St. Luke’s reported the first implantation of the BiVACOR Total Artificial Heart in a human. It is a titanium biventricular rotary pump with a single moving part: a magnetically levitated rotor. The device replaces both ventricles of the heart and is designed as a bridge to transplantation for patients with severe heart failure.
In 2025, the story became even more striking. In Australia, a patient with a BiVACOR became the first person to be discharged from the hospital with this type of total artificial heart. He lived with the device for 105 days, waited for a donor heart, and then received a transplant.
That is a real milestone. It is one thing to lie in intensive care connected to an experimental device. It is another to leave the hospital and live with it for weeks outside the ward. For now, BiVACOR is a bridge, not a permanent replacement for transplantation. But it is a step toward an artificial heart that a person could live with for years, not just long enough to reach a donor organ.
Similar work is happening in nephrology. The implantable bioartificial kidney from the UCSF Kidney Project has not yet reached clinical trials, but preclinical models have already shown that its key components can work: a filter and a bioreactor with kidney cells. Still, until clinical trials begin, it is too early to say how applicable this approach will be.
What Will the Organ Market of the Future Look Like?
The future is unlikely to look like a catalog where someone can choose a new liver. Reality will be more interesting and more complicated.

One patient may receive a donor organ preserved on a perfusion machine. Another may receive a genetically modified pig kidney because they can no longer wait for a human one. A third may get a mechanical heart as a bridge to transplantation. A fourth may receive a printed cartilage fragment or a tissue implant after an injury. A fifth may receive an organ whose “shelf life” has been extended with enzymes, perfusion, or cell therapy. And a sixth, perhaps decades from now, may receive an organ grown from their own cells.
The most realistic scenario is that there will be no single winner. There will be an ecosystem: donation, xenotransplantation, bioprinting, artificial devices, cell engineering, and smart logistics. All of this will expand classical transplantation.
This raises philosophical and ethical questions. In the past, an organ was a rare gift that became available only through a tragic chain of circumstances: someone died, someone was compatible, someone made it in time. In this new medicine, an organ is gradually becoming a technology. It can be prepared, preserved, edited, partially printed, experimentally grown, or mechanically supported.
But is it acceptable to breed animals specifically for organs? Who will get access to expensive technologies first? How should infection risks be regulated? What should count as enough evidence of safety? Could life-saving medicine turn into a market for the wealthy? Could people begin to take their health less seriously if they know replacement organs might be available?
These are not small problems. They will determine whether today’s experiments become routine medicine. Perhaps in twenty years, transplant waiting lists will still exist. But they may no longer feel like a sentence with no alternatives. Doctors may have more ways to keep a patient alive: better-preserved donor organs, genetically edited pig organs, printed tissue grafts, and artificial devices. Patients may no longer have to wait only for a night-time call from the clinic. They may have another chance — one that is being grown, printed, preserved in a machine, or built in the laboratory.