
Surgical robots are already part of modern medicine, but few people seem to realize it. The paradox is that the technology is advancing rapidly: new platforms, digital ecosystems, early clinical telesurgery protocols, and even laboratory demonstrations of partial autonomy are all emerging at once. Yet when you step into a hospital, things often look much the same as they did 5 to 10 years ago. Economics, regulation, and organizational barriers are a big part of the reason.
Robotic systems in the operating room are typically very expensive, not least because of the cost of instruments and disposable supplies. And compared with conventional laparoscopic surgery, which is far less expensive, their advantages are often modest or unclear. Bringing a robot into the operating room almost always means additional time, expense, and complexity, including training the entire surgical team and meeting evidence and post-market surveillance requirements. In recent years, cybersecurity has also become a growing concern, including the possibility that malicious actors could compromise control of the system.
To understand why, it helps to look more closely at how surgical robotics has evolved.
Major milestones in robotic surgery
It is important to clarify that when we talk about robotics in medicine, we do not mean humanoid machines independently performing surgery. In practice, we are usually talking about robot-assisted surgery (RAS): the surgeon controls the instruments from a console, while robotic arms translate those movements into precise actions inside the patient’s body. There are clear rules such systems must not perform surgery without direct human oversight and control.
Robotic surgery became possible when three technologies matured: systems for stabilizing and positioning cameras and instruments, telemanipulation, and computer-assisted planning and navigation.
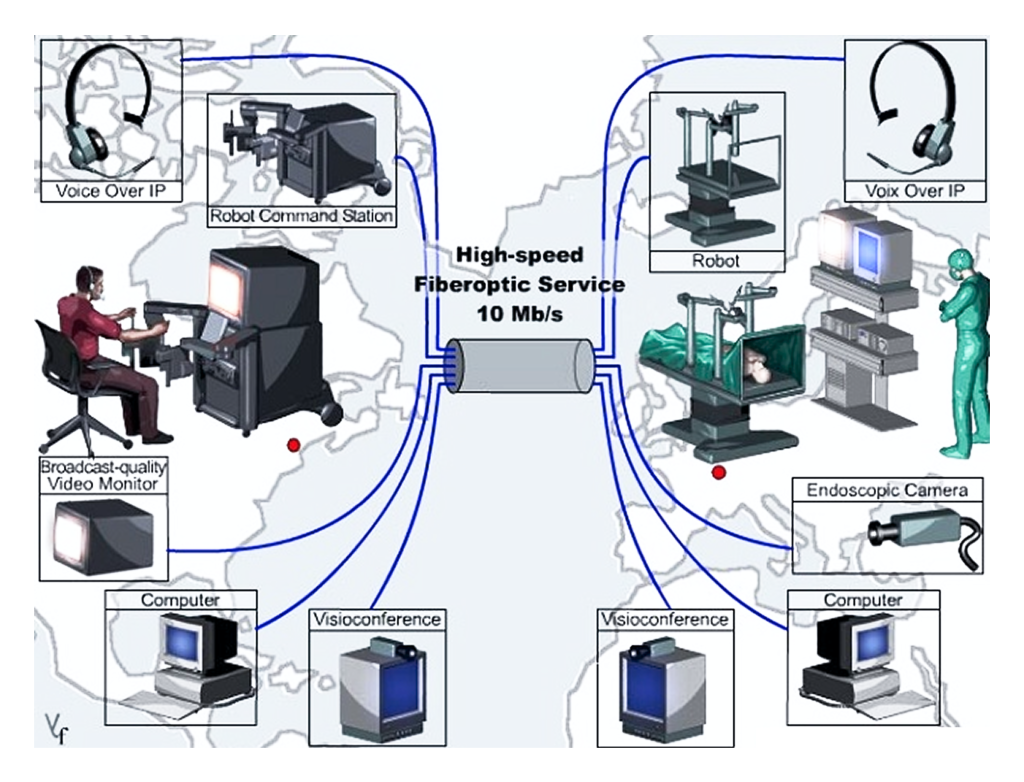
One major milestone came in 2001 with the transatlantic “Lindbergh Operation,” a landmark demonstration of telesurgery. The surgeon operated the ZEUS robotic system from New York while the patient was in Strasbourg.
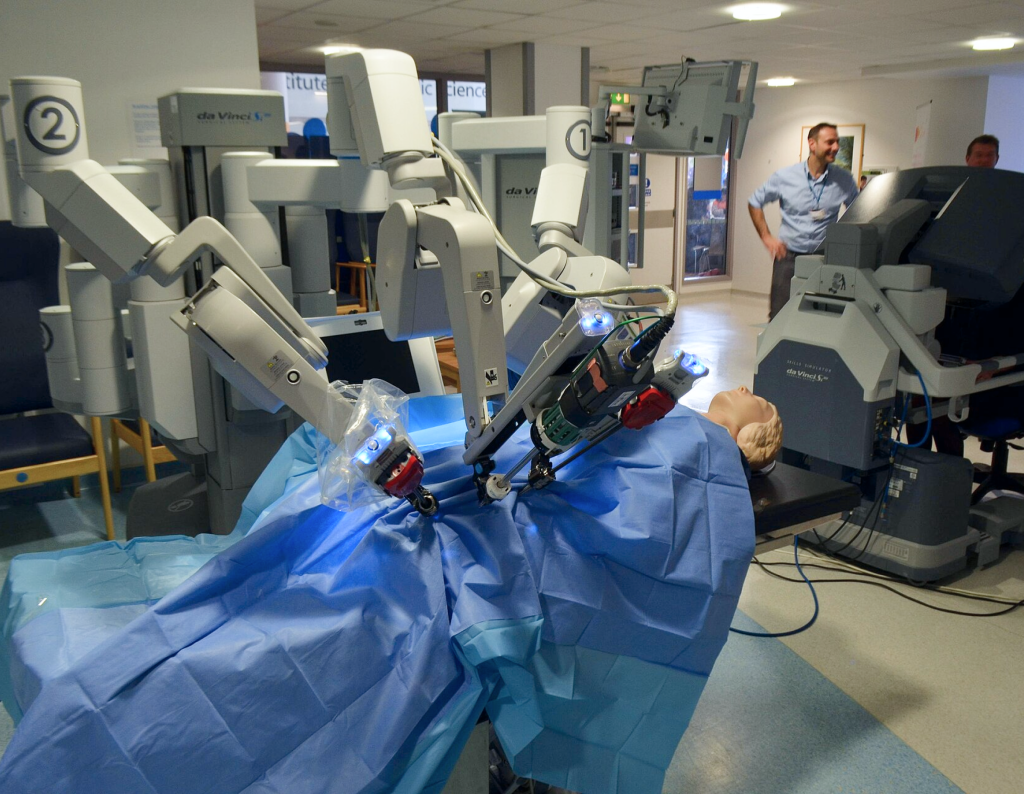
Around the same time, the da Vinci system began to gain traction. Typically, one arm holds the camera, two others control the instruments, and a fourth can assist as needed. The system gives the surgeon a magnified three-dimensional view of the surgical field.
Despite the success of these early procedures, broader adoption was held back by concerns over network stability and latency, safety, liability, cost, and legal frameworks. Even so, robotic systems continued to evolve: their capabilities expanded, the range of procedures grew, and surgeons were able to work on increasingly small anatomical structures. Some of the most striking demonstrations showed surgeons using robots to place sutures on extremely delicate targets, including the skin of a corn kernel.
In real patients, robotic systems have been used remotely for both common procedures, such as cholecystectomy and hernia repair, and more complex operations, including mitral valve repair and cystectomy.
A new phase in the field began around 2019, when several key patents expired.
What’s changing now
Today, progress in surgical robotics is being driven by new engineering approaches, the broader digitalization of the operating room, and partial autonomy, with AI increasingly acting as a kind of second pilot.
Surgical robots are changing not only in appearance, but also in how they are designed and used. Until recently, most were large, expensive all-in-one systems. Now manufacturers are exploring a wider range of formats.
One approach is the modular system. Instead of a single large structure, these systems use separate mobile arms that can be positioned around the operating table. The goal is to make the setup more flexible and potentially easier for hospitals to integrate into existing workflows. Some newer platforms, such as Hugo, follow this model. Manufacturers argue that such systems could help address some longstanding barriers in robotic surgery, especially the complexity of adoption and high operating costs. They also offer features that are increasingly standard in modern robotic platforms: 3D visualization, wristed instruments, and the ability to record procedures for later review and training.

Another important trend is the push to perform surgery through ever smaller access points. One example is the rise of so-called single-port systems, in which the instruments and camera are inserted through a single incision rather than several. For patients, the appeal is obvious: fewer incisions, less tissue trauma, less visible scarring, and potentially a faster recovery. These systems are gradually gaining approval not only for rare or experimental interventions, but also for more common procedures such as gallbladder removal, appendectomy, and inguinal hernia repair.
But one of the biggest changes is that surgical robots are increasingly being sold not as standalone machines, but as part of a much broader digital ecosystem. That ecosystem can include video capture, analysis of the surgeon’s movements, simulation tools, remote observation, and digital mentoring. Some platforms can already assess aspects of surgical performance using objective metrics.
Remote surgery
Although successful examples of surgery performed by a surgeon on another continent have existed for years, such procedures have remained rare.
For this kind of surgery to be safe, signals must be transmitted with minimal latency and extremely high reliability. Otherwise, even a slight delay or partial loss of data between the surgeon’s input and the robot’s response could put the patient at risk. Advances in 5G and satellite communications have made it possible to transmit video and commands faster and more reliably than before.
However, before remote surgery can be adopted on a large scale, standardized protocols still need to be developed, covering which communication channels are acceptable, how much latency can be tolerated, what should happen if the signal drops, how the system should be protected from failures and cyberattacks, and what the surgeon should do if the connection deteriorates during a critical stage of the procedure.
Could surgery ever become autonomous?
Today, AI in the operating room functions primarily as an assistant, not an independent surgeon. It can identify anatomical structures in an image, highlight what is visible in the field, help analyze the progress of a procedure, detect deviations from the usual course of an operation, and support quality control. But final decisions and real-world actions still remain firmly in human hands.
At the same time, laboratory and experimental studies have already shown that some surgical steps can be performed with a significant degree of autonomy. For example, in 2022, Science Robotics described a system capable of performing an intestinal anastomosis with a relatively high degree of autonomy—that is, reconnecting two sections of bowel after they have been cut. Using camera and sensor data, the robot joined the tissues according to a predefined strategy.
In 2025, a team at Johns Hopkins University reported that a robot had completed an extended portion of a cholecystectomy—gallbladder removal surgery—on highly realistic models designed to simulate the human body.
Given the pace of progress, Elon Musk said in early 2026 that autonomous robots could match the world’s best human surgeons within three years. For now, however, the main question is not when robots will fully replace surgeons. The real question is what role they will ultimately play in the operating room: whether they will remain an expensive niche tool, become reliable digital co-pilots, or eventually take over certain standardized parts of surgical procedures.